TL;DR:
- Hyperactive-impulsive ADHD involves excessive physical activity and impulsive behaviors that differ from other types. It is most often diagnosed early and is less common than the combined type, affecting about 5-10% of cases. Supporting children requires environmental adjustments, consistency, and understanding their neurological challenges rather than relying on discipline alone.
The hyperactive-impulsive type of ADHD is defined by persistent, excessive physical activity and impulsive behavior that go well beyond typical childhood energy. Clinically recognized under the DSM-5 as one of three ADHD presentations, this type stands apart from the inattentive and combined types in ways that directly shape how a child behaves at home, in the classroom, and with peers. Understanding the adhd hyperactive impulsive type differences is not just useful knowledge. It is the foundation for getting a child the right support. As of 2026, 11.4% of American students carry an ADHD diagnosis, reflecting a 65% increase since 2000. That number tells you how many families and educators are navigating this right now.

What are the key symptoms of the hyperactive-impulsive ADHD type?
Hyperactive-impulsive ADHD produces behaviors that are hard to miss. A child with this presentation does not simply have a lot of energy. The restlessness exceeds developmental expectations, meaning it is not what you would expect from any child at that age. That distinction matters because it shifts the conversation from "this child is just being a kid" to "this child's brain is working differently."
The most visible hyperactive ADHD symptoms include:
- Fidgeting constantly with hands, feet, or objects, even when seated
- Leaving their seat in class or at the dinner table when staying seated is expected
- Running or climbing in situations where it is clearly inappropriate, such as during a quiet lesson
- Talking excessively and at a pace that feels unstoppable
- Being "on the go" as if driven by a motor, with difficulty slowing down even when tired
Impulsive ADHD characteristics look different but are equally disruptive. A child blurts out answers before a question is finished. They interrupt conversations without realizing it. They grab things from others, act without thinking through consequences, and struggle to wait their turn in line or in games.
The contrast with the inattentive type is significant. A child with inattentive ADHD tends to be quiet, easily distracted, and forgetful. They may stare out the window and lose track of instructions. A child with the hyperactive-impulsive type is the opposite: loud, physical, and reactive. Both children have ADHD, but their classroom footprint looks completely different.
Pro Tip: If you are unsure whether a child's energy is typical or something more, track the behavior across two settings, such as home and school. A diagnosis requires that symptoms appear in two or more settings with clear functional impairment.
How common is the hyperactive-impulsive type compared to other ADHD types?
The hyperactive-impulsive presentation is the rarest of the three ADHD types. Understanding where it sits in the broader ADHD types comparison helps set realistic expectations for diagnosis and support.
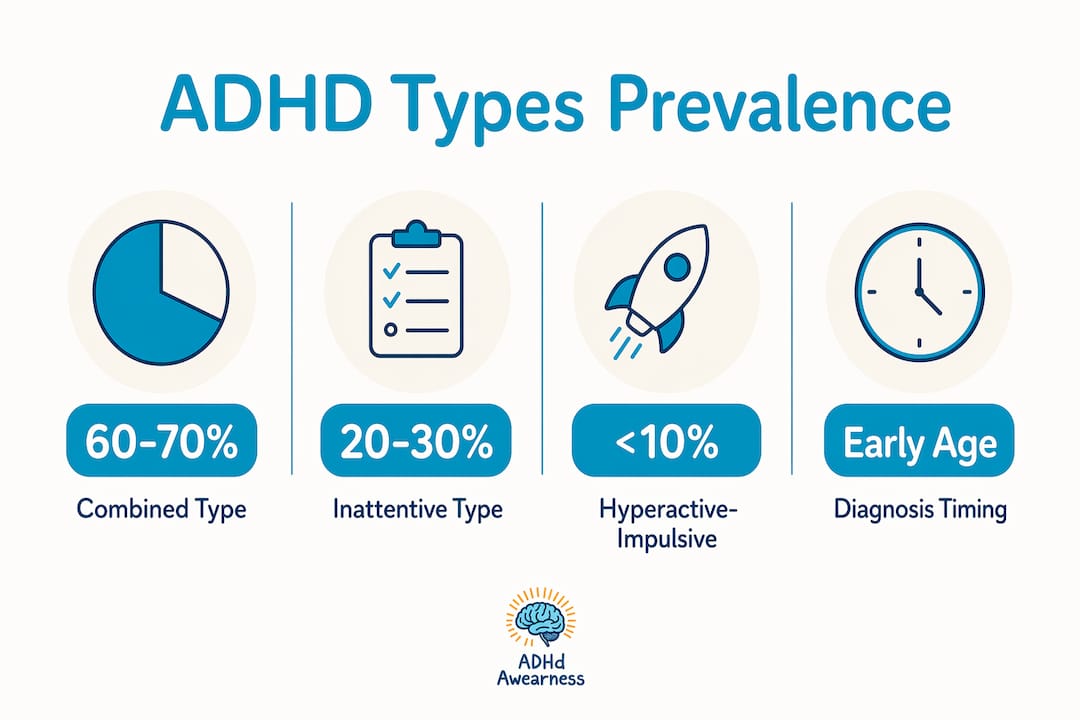
| ADHD Type | Estimated Prevalence |
|---|---|
| Combined type | 60–70% of cases |
| Inattentive type | 20–30% of cases |
| Hyperactive-impulsive type | 5–10% of cases |
The combined type accounts for 60–70% of all ADHD diagnoses, making it by far the most common. The hyperactive-impulsive type, at just 5–10%, is diagnosed far less frequently. That rarity has a practical consequence: fewer resources, fewer teacher training programs, and fewer parent guides are built specifically around this presentation.
Age plays a major role in how this type shows up. The hyperactive-impulsive type tends to be diagnosed earlier, often in preschool or early elementary school, because the physical behaviors are impossible to overlook. A four-year-old who cannot sit through circle time and runs into walls is noticed quickly. A nine-year-old who daydreams and loses homework is often missed for years.
Gender also shapes the picture. Boys are more frequently diagnosed with the hyperactive-impulsive presentation, while girls more often receive an inattentive diagnosis. This is partly because hyperactive behavior in boys draws more immediate attention from teachers and parents. Girls with the same neurological profile may be overlooked because their symptoms are less disruptive on the surface.
How does hyperactive-impulsive ADHD affect children in classroom and social settings?
The classroom is where the difference in ADHD types becomes most visible and most consequential. A child with hyperactive-impulsive ADHD does not just struggle to sit still. Their behavior ripples outward, affecting the teacher's ability to instruct and the other children's ability to focus.
Impulsivity causes peer friction through frequent interruptions and disregard for social rules. A child who grabs toys, cuts in line, or shouts over classmates is not being malicious. Their brain processes the impulse to act before the brake system kicks in. Other children, however, experience this as rude or aggressive, which leads to social rejection over time.
Children with hyperactive-impulsive ADHD often appear restless, fidgety, and have difficulty with quiet play or waiting their turn. These behaviors are neurological in origin, not a choice, and treating them as willful misbehavior makes the problem worse, not better.
The classroom environment itself plays a significant role in how well these children function. A rigid, lecture-heavy classroom with long periods of sitting amplifies every symptom. A classroom with movement built into the routine, flexible seating, and short task cycles reduces friction considerably. This is not about lowering expectations. It is about matching the environment to how the brain works.
Teachers can take several concrete steps to support these students:
- Seat the child near the front to reduce distractions and allow for quiet redirection
- Use visual timers so the child can see how long they need to stay on task
- Build in movement breaks every 20–30 minutes to release physical tension
- Give the child a job during transitions, such as handing out papers, to channel energy productively
- Use private signals instead of public corrections to preserve the child's dignity
You can find more research-based strategies in this guide on ADHD classroom behavior that covers how these symptoms play out across different grade levels.
Pro Tip: Avoid asking a hyperactive-impulsive child to "just sit still." Neurological motor impulses make it physiologically difficult to stay still even when the child wants to comply. Offer a fidget tool or allow standing at the desk instead.
How can parents and educators support children with hyperactive-impulsive ADHD?
Support works best when it is consistent across home and school. Children with this presentation need structure, predictability, and physical outlets built into their daily routine. The goal is not to eliminate their energy. It is to give it a channel.
Here is a practical framework for both parents and educators:
- Create a visual daily schedule. Post it where the child can see it. Knowing what comes next reduces anxiety and impulsive reactions to transitions.
- Set clear, short expectations. Instead of "behave at dinner," say "stay in your seat until everyone is done eating." Specific rules are easier for impulsive brains to follow.
- Use sensory-friendly seating. Wobble cushions, standing desks, and resistance bands on chair legs give the body something to do while the mind focuses. Planned movement breaks and sensory seating are proven classroom adaptations.
- Catch the child being good. Positive reinforcement works faster than punishment for impulsive behavior. Name the specific behavior you want to see more of.
- Reduce wait time. Long waits are torture for a child with impulse control challenges. Break tasks into smaller chunks with immediate feedback.
- Communicate across settings. A daily check-in between teacher and parent, even a brief note or app message, keeps both adults aligned and prevents the child from falling through the cracks.
- Pursue a professional evaluation. A pediatric psychologist or developmental pediatrician can confirm the diagnosis and recommend whether behavioral therapy, medication, or a combination is appropriate.
For classroom-specific redirection techniques, the guide on redirecting an ADHD student offers step-by-step approaches that work without disrupting the rest of the class.
Pro Tip: Behavioral therapy, particularly parent training in behavior management, is the first-line treatment recommended for children under six with ADHD. Medication is typically considered alongside therapy for older children, not as a replacement for structure and support.
What I've learned about hyperactive-impulsive ADHD that most guides miss
The biggest misconception I see repeated is that hyperactive children simply need more discipline. Parents hear it from relatives. Teachers feel pressure to enforce it. But hyperactive and impulsive behaviors are neurological, not intentional. A child cannot will their way out of a brain that fires impulses faster than their frontal lobe can process consequences. Punishing that child for something they cannot fully control does not teach self-regulation. It teaches shame.
What actually works is changing the environment before trying to change the child. When a classroom is redesigned to include movement, or a home routine is built around predictability, the child's behavior often improves without a single correction. That is not magic. That is neuroscience applied practically.
One more thing worth knowing: hyperactivity tends to decrease with age, while inattentive symptoms often increase during adolescence. A child who looks purely hyperactive-impulsive at age five may shift toward a combined presentation by middle school as academic demands grow. This is not the child getting worse. It is the brain maturing while the environment's demands outpace that maturation. Knowing this helps parents and educators stay ahead of the curve rather than being blind sided by a "new" problem.
The children who thrive are the ones whose adults understand that the goal is not compliance. It is connection, structure, and the right kind of support at the right time.
— Bruce
ADHD Awearness resources for families and educators
Understanding this type of ADHD is a real first step. ADHD Awearness exists to make that step easier for every parent and educator who needs clear, honest information without the jargon.
ADHD Awearness produces educational content, including blogs, videos, and podcasts, built specifically for families navigating ADHD in all its forms. Every piece is designed to reduce stigma and build real understanding. The ADHD Awearness store carries 100% USA-made apparel that sparks conversations and supports ADHD-focused nonprofits with every purchase. If you want to wear your support for awareness, the ADHD abilities collection is a meaningful place to start. Visit ADHD Awearness to explore all available resources and connect with a community that gets it.
FAQ
What is the hyperactive-impulsive type of ADHD?
The hyperactive-impulsive type is one of three ADHD presentations defined by the DSM-5, characterized by excessive physical activity and impulsive behavior that exceed developmental norms, without the primary inattentive symptoms seen in other types.
How does hyperactive-impulsive ADHD differ from the combined type?
The combined type accounts for 60–70% of ADHD cases and includes both inattentive and hyperactive-impulsive symptoms, while the hyperactive-impulsive type involves only the physical and impulsive behaviors, making it the rarest presentation at 5–10% of cases.
At what age is the hyperactive-impulsive type usually diagnosed?
This type is typically identified in preschool or early elementary school because the physical behaviors are highly visible and disruptive from an early age.
Can a child's ADHD type change over time?
Yes. Hyperactivity tends to decrease with age, and a child initially diagnosed with the hyperactive-impulsive type may shift toward a combined presentation during adolescence as inattentive symptoms become more prominent with increased academic demands.
What is the most effective support strategy for hyperactive-impulsive ADHD in the classroom?
Adjusting the classroom environment, including planned movement breaks, sensory seating, and short task cycles, produces measurable improvements in behavior and engagement without requiring the child to suppress neurological impulses they cannot fully control.